Introduction
Simple enough, right? So why would this topic need a whole website and simulator?
The answer is that we cannot directly measure pulsus paradoxus the way we measure blood pressure. The tools are basically the same – you’ll need a manual blood pressure cuff and a stethoscope. And once learned, the skill doesn’t take more than a few minutes to do. But just like in performing an invasive procedure, many microskills are used over the course of those few minutes, and a solid conceptual understanding helps us remember what to do and how to do it. So let’s deconstruct this thing, conceptually and then procedurally.
Pulsus paradoxus, conceptually: 3 core concepts
Core concept 1: variation in BP creates three zones of responses to cuff pressures
If the systolic blood pressure varies over a respiratory cycle (let’s say, between 120 mmHg and 130mmHg), that naturally creates three zones of pressures.
- One zone (above 130 mmHg) where the BP never gets that high – so no Korotkoff sounds will be heard when a cuff is inflated to that pressure.
- One zone (120 mmHg to 130 mmHg) within which the BP varies (so a cuff stably inflated to 125 mmHg will lead to Korotkoff sounds being heard on some cardiac cycles, but not others).
- One zone (below 120 mmHg) where the blood pressure will always remain above the cuff’s pressure, so Korotkoff sounds are always heard (assuming that the cuff pressure isn’t way lower than the systolic pressure).
Core concept 2: three zones means two transition points between zones
In the example above, the transition points are 130 mmHg and 120 mmHg.
Core concept 3: the pulsus paradoxus is the higher transition point minus lower transition point
From conceptual understanding to procedural implications
These 3 core concepts have some important implications for why it can be challenging to measure pulsus paradoxus:
- Pulsus paradoxus is not directly measured, it is calculated by subtracting two transition points.
- Those two transition points aren’t directly measured either! For example, if you heard no sounds at 130 mmHg, and heard some sounds at 126 mmHg, you know that the transition point must be somewhere between 126 and 130 mmHg. If each transition point has a possible range of 4 mmHg, the uncertainty of the pulsus paradoxus is 8 mmHg! The uncertainty is additive
- If you’re keeping score so far, that’s at least four samplings you need to take in order to make even as vague-sounding a claim as “this patient’s pulsus paradoxus was somewhere between 4 and 8”. Unfortunately, you’ll probably need to obtain even more than these four, in order to have a sufficiently precise estimate.
- Each sampling requires keeping the cuff stably inflated at a single pressure for several seconds – enough time to probe a full respiratory cycle and determine if you hear Korotkoff sounds all of the time, some of the time, or not at all. If a patient is breathing ten times per minute, that’s six seconds for a full cycle.
Pulsus paradoxus, procedurally: 3 steps
- Inflate the cuff to a blood pressure, keep it there for several seconds, and determine if you hear the sounds all of the time, some of the time, or none of the time. Jot down a note (e.g. “126 some”).
- Keep taking more samplings (at a higher or lower pressure, as appropriate) with the goal of confining each transition point to within a range of 2 mmHg.
- Calculate an upper and lower bound for the pulsus paradoxus using the method below.
Doing the math: estimating the pulsus paradoxus
After taking your samplings, you’ll end up with a list of observations, like this:
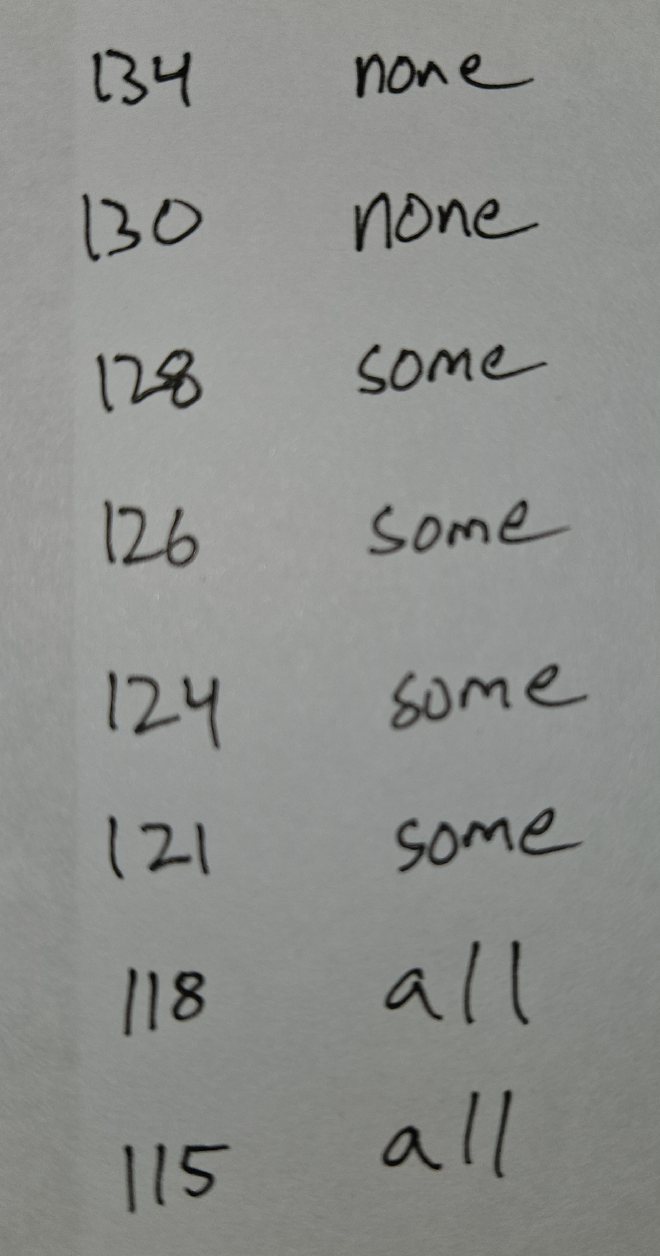
The range of possible pulsus paradoxus values is 7 to 12 based on these readings. Stop and see if you can figure out which readings are used in the calculation before reading on.
The lower bound on the pulsus is 128 - 121 = 7 (this is the highest “some” value minus the lowest “some” value). The upper bound on the pulsus is 130 - 118 = 12 (this is the lowest “none” value minus the highest “all” value).
Review
Put it into practice
You can’t learn to do this just by reading. It’s time to go practice with the simulator !